A Diagnodent Reading of 10 to 15 Indicates Which Actions?
Fig. 6.i
Visual close inspection can straight the attention in dissimilar areas of the dental surface to identify the presence of initial demineralization and/or caries; white spots on molar fissures, that are indicative of progressive demineralization stage (black arrows) (Reprinted with permission from Olivi et al. [1])

Fig. 6.2
Visual close inspection shows the presence of nighttime spots, ordinarily not associated with enamel demineralization; probing, 10-ray, and LF diagnosis will give a more than precise diagnosis
Even the periapical or bitewing intraoral 10-rays cannot show initial enamel caries (class I); the radiographs may instead be an of import aid in the diagnosis of proximal caries when carious process extends in dentin (course II and 3).
Furthermore, caries risk patients that undergo clinical checks every 3–6 months are possibly exposed to an excessive radiation dose summation, and also pregnant women cannot receive x-rays, so exploring alternative noninvasive methods is necessary.
Lasers have many uses in preventive dentistry for the post-obit purposes [1]:
-
Caries detection: laser fluorescence (LF) has been used for preoperative diagnosis of caries (DIAGNOdent, KaVo) in both main and permanent teeth and equally an intraoperative diagnostic tool (SIROInspect, Sirona).
-
Caries prevention: several infrared laser wavelengths have been used to provide increased enamel surface resistance to acrid set on as experimental methods of caries prevention.
-
Sealants: erbium lasers irradiation are used to provide enamel surface modifications that are suitable for the application of pit and cleft sealants.
vi.ii Laser for Caries Detection
Light amplification by stimulated emission of radiation for caries diagnosis is the near widely investigated light amplification by stimulated emission of radiation application in pediatric dentistry. In the terminal fifteen years, several technologies were adult and investigated for different diagnostic purposes, including preoperative, intraoperative, and postoperative diagnosis. Laser fluorescence (LF) device using 655 nm light (DIAGNOdent and DIAGNOdent-pen; KaVo, Germany) is the more than studied technology for preoperative diagnosis. Laser fluorescence at 405 nm (SIROInspect, Sirona, Germany) is a recent technology for intraoperative cheque of remaining carious tissue during excavation. The quantitative light fluorescence (QLF) uses a blueish light, while the optical coherence tomography (OCT) uses near-infrared light at 1310 nm for preoperative diagnosis. Besides the transillumination imaging diagnostic method uses laser light at 780 nm (DIAGNOcam) to produce proximal lesion images that are reported every bit comparable to bitewing radiographs.
vi.2.1 Laser Fluorescence: The DIAGNOdent
Laser fluorescence (LF) is the virtually widespread laser diagnostic technology; it is a not-ablative laser device that emits a visible, scarlet light at 655 nm.
When the light is directed towards the occlusal fissures of posterior teeth, it is easily transmitted through the enamel and is absorbed past a specific target. Effectively, bacteria by-products and porphyrins inside the carious lesion absorb and simultaneously reverberate a red fluorescent light that is detected and rated at a digital display and every bit an acoustic betoken [ii, 3] (Figs. 6.3, vi.4, and 6.5).

Fig. 6.three
LF detects with higher sensitivity and good specificity occlusal scissure caries; first the laser identifies the fluorescence value of healthy enamel (e.g., the enamel of a cusp)

Fig. 6.iv
DIAGNOdent detects and then the fluorescence of occlusal pits and fissures

Fig. six.five
DIAGNOdent registers a numerical charge per unit of the detection, reporting on the left the initial value of the healthy enamel and on the correct the actual value detected (east.g., 99 is indicative of deep dentin caries)
Iwami et al. reported the relationship between bacterial infection of carious dentin and LF detection (polymerase chain reaction). The values of the LF increased equally the leaner detection rates increased, reinforcing the concept of the relationship between fluorescence values of caries and rates of bacteria by-products and porphyrins nowadays [4]. Later, Neuhaus et al. as well reported that the quantitative measure out of fluorescence of the tooth was related more to the presence of bacterial by-products than to the mineral loss subsequent to the development of a caries lesion [5].
Several studies compared different caries detection methods: visual inspection solitary, visual inspection with magnification, bitewing x-ray, and laser fluorescence with different results.
Lussi and Francescut confirmed the very loftier reliability and the diagnostic validity (sum of sensitivity and specificity) of LF for occlusal caries detection and also reported information technology, as higher than bitewing radiography for proximal caries diagnosis in primary teeth. The authors ended that LF could exist used as an additional tool in the detection of occlusal caries in deciduous teeth and its good reproducibility should enable the light amplification by stimulated emission of radiation device to monitor the caries procedure over time [half-dozen]. Some other study reported that the reliability, predictability, and the reproducibility of the detection did non result every bit dependent on operator factor [7].
Olmez et al. (2006) evaluated the sensitivity and specificity of DIAGNOdent, visual exam, and bitewing radiography. Sensitivity measures the proportion of actual positives which are correctly identified as such (e.g., the per centum of decayed teeth who are correctly identified as having the condition). Specificity measures the proportion of negatives which are correctly identified every bit such (e.g., the pct of healthy teeth who are correctly identified equally not having the condition). Sensitivity and specificity for DIAGNOdent, visual examination, and bitewing radiography were 0.86/0.80, 0.69/1.00, and 0.36/1.00, respectively. The LF showed lower specificity than visual inspection and bitewing radiographs merely on the contrary demonstrated significantly college sensitivity for caries lesions than other conventional methods. Consequently, in case of doubtful diagnosis after clinical exam, LF having high sensitivity may be a useful offshoot to visual inspection with a loftier specificity to formulate the proper diagnosis of occlusal caries [viii, 9].
Chu et al. compared three dissimilar methods for fissure caries detection in 2nd permanent molars of young adults (visual examination, bitewing radiographs, and DIAGNOdent) and concluded that the combined approach of the LF and visual examination produced the meliorate results [10].
Diniz et al. conducted an in vivo study to determine clinical cutoffs for a DIAGNOdent, a DIAGNOdent-pen, and a DIAGNOcam (fluorescence photographic camera, FC) and to evaluate the clinical performance of these methods and conventional methods in detecting occlusal caries in permanent teeth. The International Caries Detection and Cess System (ICDAS), the LF device, and the LF pen demonstrated practiced performance in helping discover occlusal caries in vivo. BW radiography and FC had the lowest performances in helping to observe the lesions. The study concluded that occlusal caries detection should exist based primarily on visual inspection. Fluorescence-based methods may be used to provide a second stance in clinical exercise [xi] (Figs. 6.6, 6.7, 6.eight, six.9, 6.10, and 6.eleven). Recently an in vivo study reported that caries lesions may be detected more accurately past laser fluorescence devices than by clinical visual inspection [12].

Fig. half dozen.6
Occlusal view of an upper permanent molar showing dark spots on pits and fissures (Courtesy of Prof. Vasilios Kaitsas, Italia)

Fig. 6.seven
DIAGNOdent-pen start detects the healthy enamel fluorescence (e.g., the enamel of a cusp) (Courtesy of Prof. Vasilios Kaitsas, Italy)

Fig. 6.eight
DIAGNOdent-pen detecting successively the fluorescence of enamel pits and fissures (Courtesy of Prof. Vasilios Kaitsas, Italy)

Fig. six.ix
Histology of an extracted molar, presenting similar very narrow crevice with apparently intact occlusal opening; enamel caries extending in dentin is difficult to identify (Courtesy of Prof. Vasilios Kaitsas, Italy)
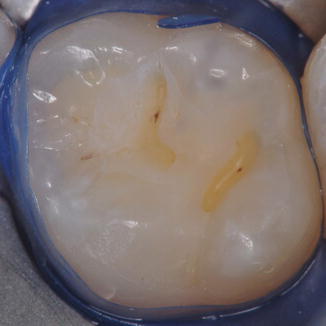
Fig. 6.10
Minimal grooming of the fissures followed the combined visual and LF diagnosis (Courtesy of Prof. Vasilios Kaitsas, Italia)
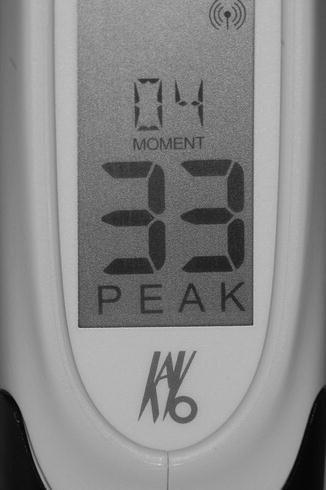
Fig. 6.11
DIAGNOdent-pen detection related to Fig. 6.8 shows loftier value pinnacle (Courtesy of Prof. Vasilios Kaitsas, Italy)
Light amplification by stimulated emission of radiation fluorescence has been proposed also for monitoring and for appropriate management of dental caries in both principal and permanent molars.
An in vitro study by Mendes et al. reported that LF was neither able to discover the remineralization of incipient caries lesions of primary teeth nor to monitor the quantification of mineral loss in caries lesion development in primary teeth [thirteen]. In a following report of the same grouping, Braga et al. reported that LF device performed better at the dentin threshold than at the enamel threshold; accordingly the study concluded that LF performed ameliorate in predicting the depth of the caries lesions (dentin caries) than the initial mineral loss (early enamel caries) [xiv].
Khalife et al. in an in vivo study also assessed the correlation betwixt the depth and volume of caries and DIAGNOdent readings and ended that the DIAGNOdent should be used just as an offshoot to the diagnosis and treatment planning procedure [15].
Also a more recent in vitro study by Bahrololoomi et al. concluded that LF is an advisable method for detection of demineralization in smooth enamel lesions, but information technology was not so efficient in the detection of remineralization [16].
Besides occlusal caries detection performed with DIAGNOdent, a more than recent version (DIAGNOdent-pen) has unlike tip shapes that enable an avant-garde proximal caries detection.
Novaes et al. compared the performance of various methods for proximal caries detection in primary molars. Both the LF pen and radiographic test exhibited like functioning in the detection of cavitations on proximal surfaces of primary molars [17].
A recent study investigated in vitro a newly developed LED fluorescence device for proximal caries detection in comparing with DIAGNOdent-pen, bitewing ten-rays, and visual inspection (International Caries Detection and Cess System, ICDAS). Reliability information scored off-white to moderate for the LED fluorescence device and good for bitewing radiography and light amplification by stimulated emission of radiation fluorescence pen. However, it is the combination of different methods that gives better results, with association of visual inspection (ICDAS) and radiography yielding the best diagnostic performance at the dentine threshold [18] (Figs. 6.12, half dozen.13, 6.fourteen, and 6.xv).

Fig. 6.12
LF detection of proximal surfaces in upper bicuspids using DIAGNOdent-pen and new tip-probe (chisel or conical) (Courtesy of Prof. Vasilios Kaitsas, Italia)

Fig. 6.thirteen
Close proximal contact betoken among 2 bicuspids hides a proximal caries that is non visible at visual inspection or probing but is detected by LF (Courtesy of Prof. Vasilios Kaitsas, Italy)

Fig. 6.14
Initial opening of cavity from occlusal ridge shows the proximal caries (Courtesy of Prof. Vasilios Kaitsas, Italy)

Fig. 6.15
The cavity preparation is completed with conventional instruments (Courtesy of Prof. Vasilios Kaitsas, Italy)
Several studies investigated detail factors that could negatively influence the detection and must be kept in heed when combining the visual inspection and laser fluorescence detection.
The presence of brownish or dark spots on fissures tends to overscore specific discolored areas of fissures, giving false positive detection [19].
The presence of plaque or toothpaste residual after teeth cleansing worsens the functioning registering false readings [20, 21]; therefore, a careful preparation must precede the laser detection.
The laser reading nether whitish dental sealants is unreliable due to inaccurate detection caused by intrinsic fluorescence of sealant material [22, 23]. However, it has been recently reported the possibility of monitoring the sealant procedure over time, when articulate sealant is used [24].
To conclude this brief overview on light amplification by stimulated emission of radiation diagnostic device guidelines, a written report by Mendes et al. was included to give a consummate and objective point of view. This study reported that adjunct methods of caries detection would non significantly amend the detection of primary molar lesions in comparison to visual inspection alone. The sensitivity, specificity, accuracy, and utility of diagnostic strategies were calculated. Simultaneous combined strategies increased sensitivities but decreased specificities, and, furthermore, no differences were observed in accuracy and utility, parameters more influenced by caries prevalence. The study concluded that present clinical guidelines should be re-evaluated [25]. In agreement with other studies [xi, 18], information technology is personal opinion of the author that LF may exist considered a valuable tool in combination to visual inspection, for caries detection as well as for longitudinal monitoring of caries and for assessing the result of preventive interventions during recall session in caries take chances patients; LF allows to space out the x-ray examinations, so reducing the radiation dose summation (Tables 6.1, 6.two, and 6.3).
Table vi.1
Shows the DIAGNOdent values of occlusal fissures detection
| DIAGNOdent™ readings according to the manufacturer |
|---|
| 0–10 = Healthy molar structure |
| 11–20 = Outer half enamel caries |
| 21–29 = Inner one-half enamel caries |
| thirty+ = Dentin caries |
Table half-dozen.ii
Shows the DIAGNOdent-pen values of occlusal fissures detection
| DIAGNOdent-pen™ readings according to the manufacturer |
|---|
| 0–12 = Healthy tooth structure |
| thirteen–24 = Outer half enamel caries (initial demineralization) |
| >25 = Inner half enamel caries (severe demineralization) |
Table half dozen.3
Shows the DIAGNOdent-pen values of proximal detection
| DIAGNOdent-pen™ readings according to the manufacturer |
|---|
| 0–seven = Healthy tooth construction |
| eight–15 = Initial demineralization |
| >xvi = Severe demineralization |
6.two.two Light amplification by stimulated emission of radiation Fluorescence: The SIROInspect™
Bacteria nowadays in the infected carious dentin release metabolic products (porphyrins) that emit visible ruby-red fluorescence when lighted with a violet laser light (405 nm). Salubrious tooth tissue differs in this respect by fluorescing greenish.
During caries digging, i of the main problems is to avoid over-earthworks saving salubrious dentin to be removed. This is too more of import when approaching deep caries for the possibility to create a pulp exposure (this topic is discussed in Sects. 7.7.2 , seven.seven.3 , and 8.ii.iii ). SIROInspect utilizes a patented engineering (FACE, fluorescence-aided caries earthworks) to illuminate the tooth cavity with violet low-cal (405 nm). The reward of intraoperative light amplification by stimulated emission of radiation fluorescence technology is that the dentist can see which areas are carious and which are not, during excavation with a much greater degree of certainty than with dye detector or visual inspection or tactile feedback lone.
The lite is delivered through a handy probe that presents an attachable filter fit and aligned on it (Fig. vi.xvi); this allows to filter out light with wavelengths below 500 nm, making the light with higher wavelengths to remain visible when the molar is exposed to violet light. Few studies are nowadays in literature on this topic.

Fig. 6.16
SIROInspect with orange filter fit on the probe

Fig. half-dozen.17
First upper quadrant of patients underwent to sealant application on bicuspids and molars 25 years before. The follow-upwards permits to check the sealing of the teeth and propose the constructing removal (microcrack on distal wall)
The studies of Lennon et al. investigated the ability of fluorescence-aided caries excavation (FACE) to discover and remove infected dentin in primary teeth compared to conventional methods (tactile excavation criteria or a caries detector dye). The quantitative confocal microscopy and histologic investigations showed significantly less remaining infected dentin in Confront samples compared to conventional digging, resulting in more effective excavation than conventional in removal of infected dentin [26, 27]. The author's experiences are very positive on the utility of this device every bit an adjunct valuable musical instrument to perform minimal invasive crenel preparation.
vi.iii Pit and Fissure Handling
Most of the increased dental caries in children and adolescents are confined to pit and fissure surfaces of beginning molars. Sealants are ane of the methods of primary prevention of dental oral diseases introduced in the 1960s, specifically to prevent fissure decays of posterior teeth [28–31]. Sealants make full the fissures of the dental surface closing the access into the deep enamel crevice of residual food and bacteria, preventing the possible carious procedure to brainstorm, and therefore is a recommended preventive process for all the children.
A systematic review conducted in 2013 reported the efficacy of sealant in reducing caries upwards to 48 months when compared to no sealant groups; however, later a longer follow-up period the quantity and quality of the evidence is reduced [32]. Therefore follow-up sessions are fundamental for monitoring the conditions of teeth in young patients and to perform the prompt corrective measures (Figs. half dozen.18 and 6.nineteen).

Fig. six.eighteen
Second upper quadrant of patients underwent to sealant application on outset bicuspid, PRR on second bicuspid, and blended restoration on first molar 20 years before. The follow-up permits to check the sealing of the teeth and to diagnose proximal decay on second molar

Fig. 6.19
Buccolingual hemi-section of recently extracted third molar shows a very narrow anatomy of the fissure
Likewise topic fluoride varnishes have been extensively used as adjunct measures to forestall dental caries in caries risk patients. In 2013 an updated review confirmed the caries-inhibiting event of fluoride varnish in both permanent and primary teeth; nevertheless, the quality of the evidence assessed was moderate [33].
In 2010, another systematic review compared the effectiveness of pit and fissure sealants with fluoride varnishes in the prevention of dental decay on occlusal surfaces. The results of the study reported show on the superiority of pit and fissure sealants over fluoride varnish application in the prevention of occlusal decay [34].
Appropriately, the application of sealant is the preventive procedure of choice for all the children. The application of fluoride varnishes could follow after some weeks of the application of sealant, to reinforce the smooth and proximal enamel areas that cannot be protected by the sealant. Fluoride varnish can exist applied periodically every 3–vi months in case of high-risk patients with poor nutrition and bad oral hygiene habits and attitudes (see Sect. 2.4.1 ). It must be emphasized that fluoride inhibits the polymerization of the adhesive and composite systems and cannot be used before, only rather must follow the adhesive procedures.
Because the different anatomy of dissimilar fissures, unlike pretreatment enamel techniques are used earlier the application of sealants Figs. 6.17, 6.xviii, 6.19, half dozen.20, six.21, and 6.22:

Fig. 6.20
Buccolingual hemi-section of extracted third molar shows a narrow good for you fissure
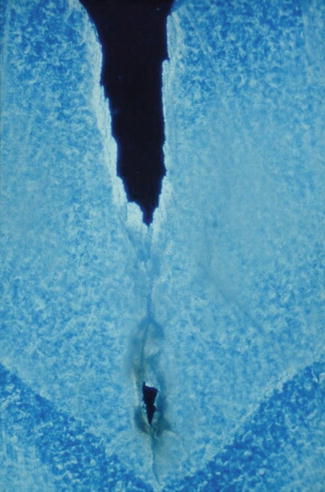
Fig. 6.21
Buccolingual hemi-section of extracted third molar shows a fissure with demineralization in depth very close to the enamel-dentin junction
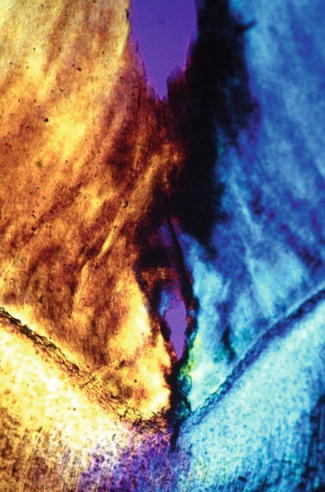
Fig. 6.22
Buccolingual hemi-section of extracted 3rd molar shows a crack with demineralization in depth very close to the enamel-dentin junction
-
Noninvasive techniques using acid etching of the occlusal fissures
-
Noninvasive techniques using air chafe followed by 37 % orthophosphoric acid etching of the occlusal fissures
-
Invasive techniques using diamond bur and high-speed drill to open up the narrow fissures (fissurotomy), followed by the etching procedure with 37 % orthophosphoric acid.
When the occlusal surface presents small fissure and/or pit caries, a selective removal of any affected enamel and/or dentin without any preparation of the neighbor intact fissures is the treatment of pick. The prepared crenel is restored with composite resin, and a sealant is placed over the remaining intact fissures and pits, completing the minimally invasive procedure with a preventive procedure for the remaining healthy enamel. This technique was introduced past Simonson and is called preventive resin restoration (PRR) technique [35].
half-dozen.iii.1 Laser Assisted Fissure Sealant (LAS)
Although in that location is testify of sealants' effectiveness, one major obstacle on its use is the concern of sealing over active caries lesions, and the conclusion of whether or not to place a sealant depends largely on the dentist'due south cess of the depth of the occlusal fossae (Figs. 6.23, 6.24, 6.25, and 6.26). Effectively pediatric dentists' perception (visual exam and tactile perception) of fossa depth in permanent molars correlates moderately well with the actual fossa depth [36], and then that clinical and anatomical consideration in combination with laser diagnostic values must exist considered earlier the sealant process, because they condition both the clinical option and the operative procedure, making the treatment plan more reliable (Figs. 6.27 6.28, 6.29, vi.30, vi.31, and six.32). Anatomical and clinical considerations include the following:

Fig. vi.23
Buccolingual hemi-department of extracted third molar following 24-h dye awarding. Image of fissure conditioned with orthophosphoric acid and sealed with no filled resin

Fig. 6.24
A magnification of the previous epitome shows presence of dye under the sealant as for initial enamel demineralization in the depth of the crack; dentin is not involved in the procedure
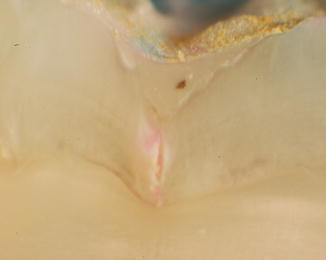
Fig. 6.25
Buccolingual hemi-section of extracted third molar post-obit 24-h dye application. Image of fissure conditioned with orthophosphoric acid and sealed with no filled resin

Fig. 6.26
A magnification of the previous image shows traces of dye nether the sealant, in the depth of the fissure that as well present initial demineralization of the enamel (clear area); dentin is not involved in the process

Fig. 6.27
Occlusal surface of extracted upper tertiary tooth presenting complicated crack beefcake; also white demineralization areas are visible

Fig. 6.28
Occlusal surface of extracted lower tertiary molar presenting complicated fissure anatomy; also white demineralization areas are visible
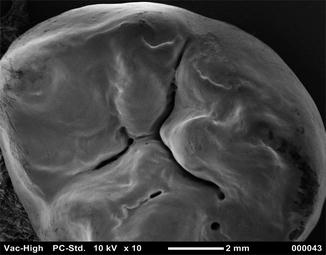
Fig. half dozen.29
SEM images (10×) of occlusal surface of upper third molar presenting complicated crack anatomy
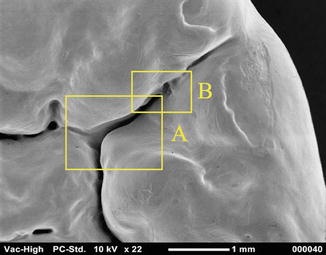
Fig. six.30
SEM images (22×) of the same tooth bear witness the influence of the magnification on the visual inspection. Iii different areas (A, B) are deeply explored
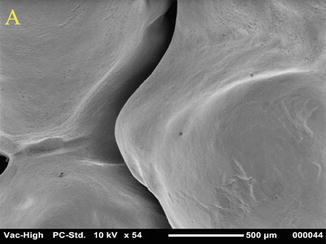
Fig. vi.31
SEM images (54×) of the A expanse of Fig. 6.30. The narrow anatomy of the tooth is clearly visible by magnification
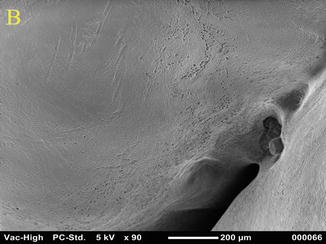
Fig. half dozen.32
SEM images (90×) of the B area of Fig. six.30. The narrow and deep beefcake of the tooth explains the difficulty in cleaning the scissure before the sealant application
-
Age of the tooth eruption (just erupted or erupted for several months or years)
-
Visual perception of pit and crack anatomy (deep, retentive)
-
Presence of dark or white spot on the fissures (demineralization)
-
LF values between 0–xx and 0–24 (DIAGNOdent or DIAGNOdent-pen*)
LF permits to diagnose the condition of the scissure and pits, addressing the procedure towards a preventive or therapeutical treatment (see Tables 6.1 and half dozen.two) (Figs. six.33 6.34, 6.35, half dozen.36, 6.37, and 6.38).

Fig. 6.33
Clinical intraoperative image shows apparently salubrious second bicuspid and first molar of a 13-yr-old boy, earlier sealant application

Fig. half dozen.34
DIAGNOdent-pen fluorescence detection of the enamel of mesial cusp

Fig. vi.35
DIAGNOdent-pen fluorescence detection of the fissures to assess the type of fissure treatment before sealant awarding
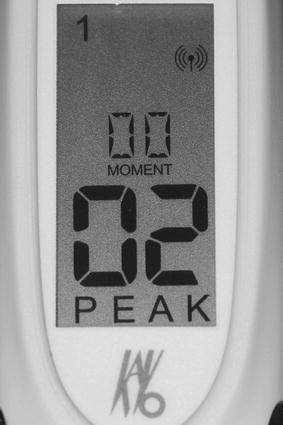
Fig. 6.36
DIAGNOdent-pen detection value of healthy enamel
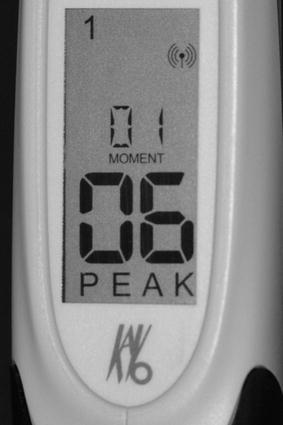
Fig. 6.37
DIAGNOdent-pen detection value of the salubrious crack
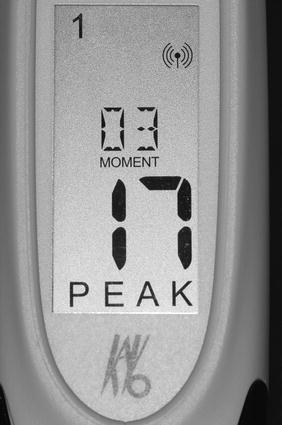
Fig. vi.38
DIAGNOdent-pen detection value of the initially demineralized fissure
When fluorescence diagnosis is combined with erbium lasers (2780 and 2940 nm), it is possible to individualize (personalize) the treatment of the scissure. Erbium lasers tin exist used as:
-
Noninvasive technique for conditioning pretreatment of healthy pits and fissures earlier acid etching and sealant (LAS) (see Table half-dozen.4)
Table 6.iv
Suggested parameters for use laser assisted crack sealant (LAS)
Accurate diagnosis of the fissures: inspection and probing nether magnification and fluorescence detection (value refers to DIAGNOdent-pen*, KaVo)
Healthy fissures
Fluorescence detection values: 0–10 (0–12*)
Appropriate energy/fluence in order to cleanse and condition: 35 > 50 mJ–20 Hz
Loftier air/water spray – short pulse duration – pulse rate may be increased if needed
Fissures with initial demineralization
Fluorescence detection values: 11–20 (13–24*)
Appropriate energy/fluence in social club to cleanse, condition, and decontaminate
Decontamination (first): 75 mJ–xx Hz
Cleansing and conditioning: 35 > 50 mJ–20 Hz
Loftier air/water spray – curt pulse duration
Accurate irradiation of fissures includes: right focus, correct inclination, precise irradiation in society to avoid irradiation of the healthy enamel of ridges, and cusps using small diameter tip >400–600 μm tip. Shut contact handpiece allows a amend control and precision
-
Minimally invasive technique for decontamination and conditioning pretreatment of deep fissures or with initial demineralization before acid etching and sealant (LAS) (see Tabular array 6.4) (Figs. six.39, 6.forty, 6.41, 6.42, 6.43, 6.44, and 6.45)

Fig. 6.39
Rubber dam application before the clinical procedure

Fig. half-dozen.40
Er,Cr:YSGG light amplification by stimulated emission of radiation irradiation of pit and fissures before sealant application: different parameters permit to differently condition or minimally prepare different areas, according to LF values detected
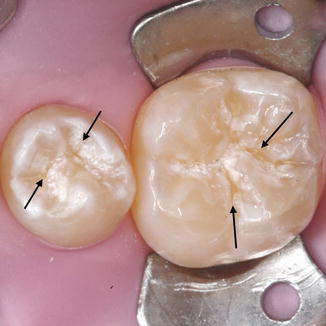
Fig. 6.41
The black arrows show the deeper and wider surface area of fissures with college LF detection values that were treated at higher fluence (ablation)

Fig. half-dozen.42
Orthophosphoric acid carving following light amplification by stimulated emission of radiation conditioning and ablation permits to improve the enamel pattern for bonding

Fig. 6.43
After acid carving the lased surface appears more make clean and uniform before sealing. The black arrows bear witness the exposed dentin subsequently laser irradiation and more axiomatic after orthophosphoric acid etching
Just gold members tin go along reading. Log In or Register to proceed
Source: https://pocketdentistry.com/laser-applications-for-caries-diagnosis-and-prevention/
0 Response to "A Diagnodent Reading of 10 to 15 Indicates Which Actions?"
Postar um comentário